So, before moving on to life in Thailand a recap of my last year in Zanzibar (this is Nadine by the way), after leaving the VSO post. Finally John can stop twisting my arm 🙂
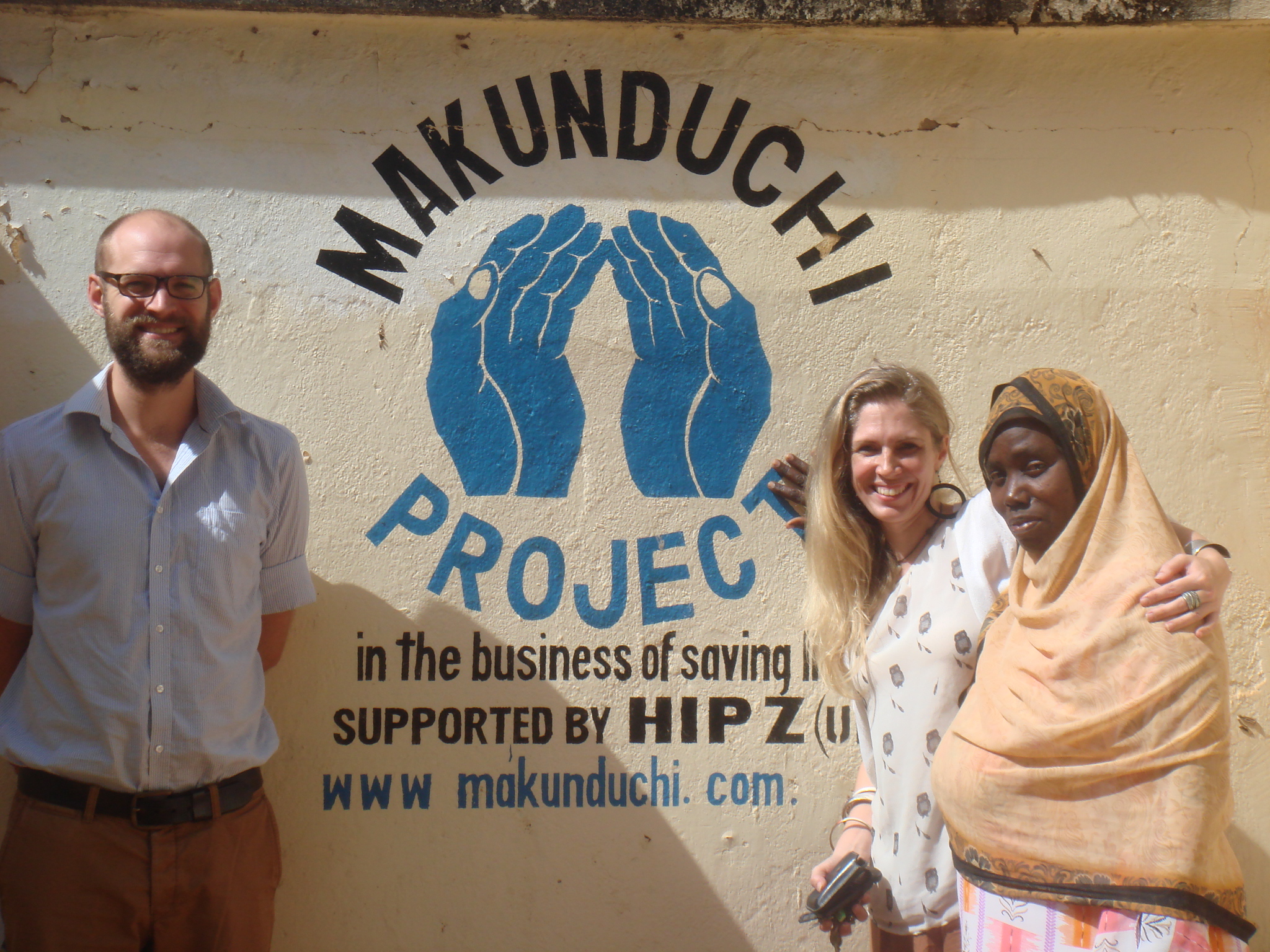
Having worked with all hospitals in Zanzibar on introducing tele-medicine within our voluntary placement we came across HIPZ (Health Improvement Project Zanzibar), a UK NGO running and improving the standards at the two rural government hospitals on the main island of Zanzibar, Unguja – over a ten year period before handing the hospitals back over to the government. HIPZ have been working in the Southern hospital in Makunduchi (with a catchment area of about 60,000 people) since 2007.

Makunduchi Hospital
As things progressed really well down there the President of Zanzibar himself requested HIPZ to take on the second rural hospital in the North at Kivunge in 2012 (which has a much bigger catchment area of about 150,000). A position to run HIPZ’ operations in Zanzibar came up in 2013, and I applied for it.
Why? Well, for some very specific reasons (only partly mentioned in John’s rant post a couple of weeks ago) we were getting a wee bit jaded with our VSO placement and this seemed like a chance to be doing development work with at least some impact. It was clear that something had been going right over the past years at Makunduchi hospital, so why not become a part of that, learn and hopefully contribute a bit, too.
What seemed different: This was not an initiative injecting vast amounts of money blindly and insensibly. a) There wasn’t that much money going round within the organisation and b) it’s just not part of HIPZ’ ethos anyway. In keeping with that no one working for HIPZ in Zanzibar has a big fancy four-by four or a villa by the sea. Actually most people involved with the organisation work entirely for free, only four people earn a very modest salary.
Two of these are the local Hospital Managers, which in a very wise move have been instated in the hospitals by HIPZ to lead on administration (although there are still major issues with getting them recognised within the government system). Seems a no-brainer, a Hospital Manager, doesn’t it? Well, Zanzibar, has an impressive number of 15 or so practising local medical doctors serving a population of well over a million. Given this excellent ratio it is rather wise of the government to request its often one and only doctor or Assistant Medical Officer at a hospital dealing with up to 350 patients a day to manage and administrate the whole place, too. That involves running off at least once or twice a week at short notice to attend seemingly endless Ministry meetings (a lunch and often a “per diem” payment is involved, so actually well worth it for the individual).
And, have I mentioned that the official minimum requirements for a so-called Cottage Hospital regarding staff are a couple of Assistant Medical Officers – let me spell it out: no qualified doctor needed! Ever thought there was a hospital – even a rural one – that is designed to offer a professional service without the presence of a doctor?
Anyway, it was my job to lead on specific projects, liaise with ministry, partners and donors, and oversee the work of the hospital managers and the volunteer doctors. They are fabulous young doctors from the UK towards the end of their training, who work for free for 6 months to a year and like us live in simple accommodation, that means no warm water, no air con, regular power outages, far too many spiders and cockroaches :-). They are suddenly faced with the massive responsibility of in effect (but alas without formal authority – I could write a book about this issue) being the clinical lead for an entire hospital, no peers or well-qualified technical staff to rely on, and very few tools to diagnose and treat patients with. Think: no ECG, no MRT, no computer tomography, no guaranteed X-ray or ultrasound, not even your basic Full Blood Count (blood tests we could get in a wink for minor complaints), sometimes not even oxygen on offer. But without all of this support they are nevertheless encountering severely sick patients on a daily basis. And the referral hospital they can send them too will most probably not offer better care. A really tough situation.

Drying X-rays on the fence

Us chilling with fab doctors
And so we all basically got involved in any aspect of hospital management in addition to medical support – doctors only for the medical stuff, that is. Unlike some of the local administrative (!) staff I decided discussing X-rays and diagnosing patients wasn’t really my cup of tea. Although I’m sure they would have let me give it a shot!

Kivunge Hospital male ward – in dire need of renovation!

Renovated children’s ward at Kivunge Hospital, mainly for malnourished babies
Improvements are addressed wherever possible at a sustainable structural level, rather than on an ad hoc basis (one-off medicine donations for example). So that would involve for example securing 24 hour availability of the ambulance for transfers to the tertiary hospital and trying to find out what’s happening to the petrol made available for this service, regularly leaving the ambulance immobile towards the end of the month. Pity that many of the ambulance drivers, who are supposed to track their patient transfers to the tertiary hospital in a log book, actually have not been taught how to read or write. And there are many other tricky issues that make getting this one to work a real challenge.
We also looked into improving the drug supply chain, as for example patients with high blood pressure would often only be 2-3 weeks a month on medication provided by the government at the hospital, the rest of the time off it – with potentially fatal effects. The idea there was to ensure a regular supply of 4 different types of anti-hypertensives via our organisation. This was then supposed to be sold off without a profit at the hospital whenever the free government supply had run out. Sounds simple but is still not up and running as far as I know. Barriers? Ensuring regular supply of drugs even in small quantities from the Tanzanian mainland seems next to impossible. Will the pharmacist manage to work with two piles of medicine – the government one and the HIPZ funded one, and know when to switch from one to the other? Also a challenge to set up. And one of the biggest concerns of hospital management: Even though we obtained an official certificate from the Zanzibar Food and Drugs Board to sell the drugs within a clearly outlined process, many people at the hospital were saying it will look like employees are doing dodgy things, selling drugs to make a private profit. Can you blame them of being afraid when this is actually happening on a regular basis across the islands?
Other things we focussed on: Fundraising for and purchasing essential equipment, renovations and new buildings…..

Spanking new outpatient department at Kivunge Hospital – weyhey, it’s finished!!
….and training, training, training.

On-the-job training by a visiting surgeon in Kivunge’s new operating theatre
And this is again where HIPZ are very different from other organisations. We are based at the hospitals with the doctors there every day, building relationships with the government-employed personnel, keen to understand the challenges, able to judge quite well what kind of innovations are feasible, and plan all aspects of their implementation. So a holistic, ‘horizontal’ approach. Most big players in the field have a ‘vertical’ approach with a focus on and insight into specific issues only: HIV, Malaria, diabetes, disease prevention, child health for example. And the truth is they don’t know the institutions all that well that they are working with and therefore have a reduced insight into what is actually required to implement changes. Plonking a piece of equipment in a hospital alone certainly has no impact whatsoever…..
So, coming back to HIPZ: What’s so different then in Makunduchi, where they have been based for seven years now? Well, for a start all in-patients are now seen on a ward round every day and have a filled-in observation chart and a drug chart. A massive improvement. I need to explain that people are terrified of being admitted to hospital. They will happily queue for hours for outpatient treatment at the facility but will do everything to avoid staying in hospital. Not a surprise as Zanzibaris traditionally equate hospital admission with being left to fester and more or less certain death. You can’t blame them. But things at Makunduchi have been changing. Some examples:
- Every day a morning meeting is held at 7:30 a.m. to do a handover from night shift, discuss difficult cases and often even get a few minutes of training on a specific issue in there
- An ambulance service has been introduced to pick up women in labour from distant villages
- Midwives fill in a partogram monitoring each woman’s labour to reduce the risk of complications.
- All mothers and newborn babies get checked by medical personnel within 24 hours of giving birth
- It has been reported from a neighbouring village that the changes at the hospital have truly transformed the life of the villagers: Since the volunteer doctors have been working closely with local staff patients are no longer afraid of being shouted at or abused when being treated. They are actually happy to come to the hospital….
Overall, and most importantly in my opinion, Makunduchi has achieved what I have seen nowhere else in Zanzibar: Staff are not a bunch of individuals looking out for themselves only. They are a team that works together and feels responsible and proud to be offering a good service. Well done to Zainab (Hospital Manager) and all the others who have contributed to this over the past seven years!!
So, if you are still looking for a way of giving back over the Xmas period I can vouch personally for any donations to HIPZ. They will be used responsibly and directly benefit the people of Zanzibar.You can donate here: https://www.justgiving.com/hipz/donate/
But now it’s high time to say kwa heri, Zanzibar, good bye, fare thee well…

And Thailand, here we come, wehyhey 🙂